
Chrysotile asbestos, a mineral once lauded for its resilience and versatility, now stands as a notorious agent of occupational and environmental health concerns. This silicate mineral, characterized by its unique fibrous crystalline structure, was extensively utilized across various industries until revelations about its hazardous effects to human health took center stage. In this essay, we will embark on a journey through the intricate world of chrysotile asbestos—from its inherent properties which once made it a material of choice, to the insidious health risks it poses upon exposure and inhalation. By delving into the body’s natural defenses and their capacity to combat the invasion of these tenacious fibers, we gain insights into the continuous battle waged within the human lungs and the ceaseless efforts to protect our respiratory health.
Properties of Chrysotile Asbestos
Title: Chrysotile Asbestos: A Distinct Mineral Fiber Among Asbestiform Silicates
Within the mineralogical kingdom, asbestos denotes a group of naturally-occurring fibrous silicate minerals that have historically played a role in various industrial applications due to their desirable physical properties. However, it is critical to discern between different forms of asbestos, particularly chrysotile, which distinguishes itself from other asbestos minerals both structurally and chemically.
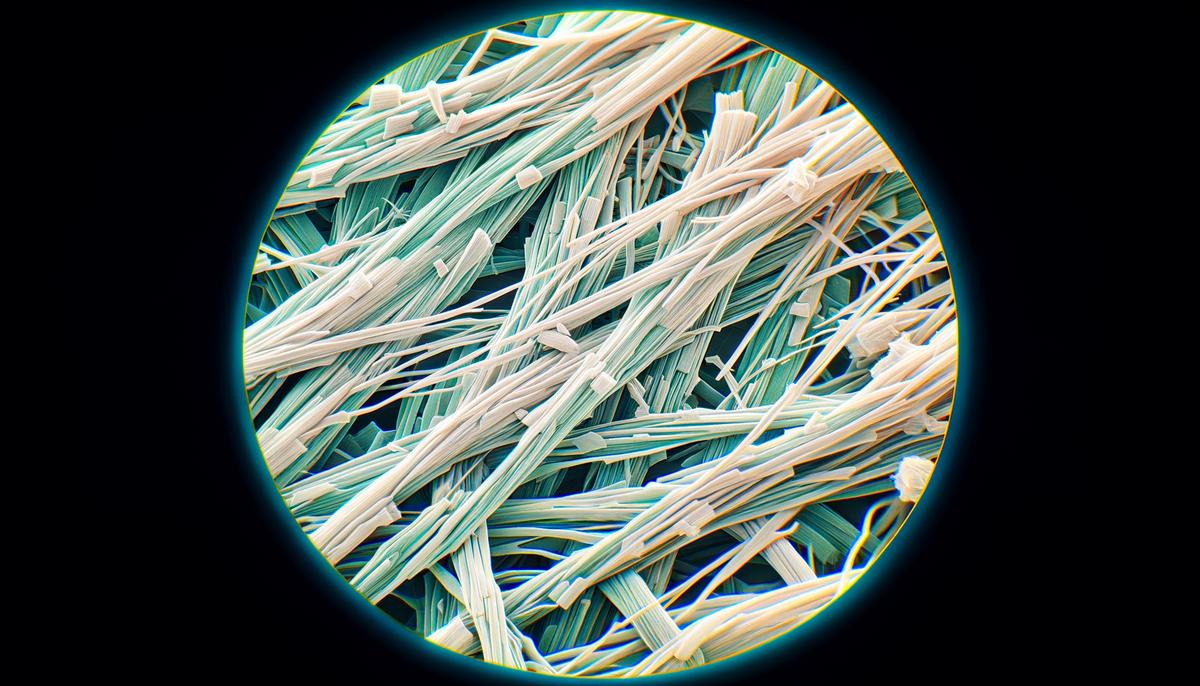
Chrysotile, commonly referred to as “white asbestos,” is the most prevalent type exploited commercially. Its fibers are composed of silicate sheets wrapped into a tubular structure, a unique trait not observed in other forms of asbestos, which possess a chain-like structure. This distinction has significant repercussions on chrysotile’s physical and thermal characteristics.
Unlike amphibole asbestos varieties – which include amosite, crocidolite, and others, known for their rigid, straight fibers – chrysotile fibers exhibit flexibility and a curved shape. This filamentous nature allows chrysotile to be spun and woven in a similar fashion to textile fibers.
Chemically, chrysotile asbestos is primarily composed of magnesium silicate, whilst amphibole asbestos contains iron and magnesium. A fundamental difference lies in their classification based on their crystalline structure; chrysotile belongs to the serpentine class, characterized by layered or sheet-like crystals, in stark contrast to the amphibole class, with a double-chain structure.
Although chrysotile’s attributes may lend it to seemingly safer handling given its lower biopersistence relative to amphibole forms, it is imperative to recognize that all asbestos types are classified as carcinogens, and their fibers can cause serious health issues upon inhalation. The mineral’s inherent risks, particularly mesothelioma and lung cancer, underline the global trend towards cease of use and safe removal of existing asbestos-containing materials.
In summary, the distinction between chrysotile asbestos and other forms of the mineral hinges on its serpentine crystalline structure, flexible and curved fibers, and specific chemical makeup. Despite its unique properties, it is essential to approach chrysotile with the same caution as other asbestos fibers, prioritizing health and environmental safety above its industrial utility.
Mechanisms of Pulmonary Clearance
Human lungs possess a remarkable and sophisticated defense mechanism that enables them to naturally clear inhaled particles, including various types of dust, bacteria, and pollutants. This process is essential for maintaining respiratory health and preventing the buildup of potentially harmful substances in the lung tissue.
The primary line of defense against foreign particles in the respiratory system is the mucociliary escalator. This mechanism involves two crucial components: mucus and cilia. Mucus, a sticky secretion produced by the goblet cells in the respiratory tract, traps inhaled particles. The cilia, hair-like projections lining the majority of the respiratory tract, beat in a coordinated rhythmic manner to propel the mucus, along with the trapped particles, upward towards the pharynx.
Once the particle-laden mucus reaches the pharynx, it typically merges into the digestive tract, where it can be neutralized by stomach acids or expelled through the act of coughing. This system operates continuously, serving as an internal air purifier that is both effective and efficient.
In addition to the mucociliary escalator, alveolar macrophages play a vital role in particle clearance within the deeper parts of the lungs, particularly in the alveolar region, where gas exchange occurs. These specialized immune cells engulf and digest foreign particles that have escaped the upper airway defenses, ensuring that the gas-exchanging surfaces of the lungs remain clear. These macrophages then either move toward the ciliated airways to be expelled or get absorbed by the lymphatic system.
Moreover, the nasal passages, as the first point of contact with the external environment, utilize nasal hairs and a layer of mucus to filter larger particles before they can penetrate deeper into the respiratory tract. Sneezing, an involuntary response triggered by irritation in the nasal cavity, serves as a sudden and powerful mechanism to expel foreign substances from the upper airways.
Overall, the human respiratory system has evolved a multi-tiered defense against the daily inhalation of particles. While this system is incredibly efficient, it is not foolproof, and excessive exposure to harmful particles, such as asbestos fibers, can overwhelm these natural defenses, leading to adverse health effects. Therefore, understanding and respecting the limitations of the body’s natural cleaning mechanisms is crucial to protect lung health in the face of occupational hazards and environmental contaminants.
Chrysotile Fibers and Lung Retention
The implications of chrysotile fibers for lung retention and potential diseases are a topic of particular concern and rigorous scientific inquiry. Due to the fibrous nature of chrysotile, it can become lodged in the alveoli and lung tissue when inhaled. Unlike other forms of asbestos, chrysotile fibers are more pliable and less needle-like, which has led to a longstanding debate about their risk profile. However, the consensus among researchers is clear: even though chrysotile fibers are serpentine and thus may be less biopersistent than amphibole asbestos fibers, significant exposure can lead to serious health consequences.
Once chrysotile fibers enter the lung, they can evade the mucociliary escalator, which is less effective for fibers than for other types of particulate matter. These fibers can remain in the lung tissue due to their size and shape, which inhibit expulsion. Over time, the presence of these fibers can lead to inflammation, cellular damage, and a disruption of normal cellular and tissue architecture.
Chronic inflammation is a precursor to fibrosis, or scarring, which is a hallmark of asbestosis. Although less common than its amphibole counterparts, chrysotile-associated asbestosis presents a significant health risk. As fibrotic lung tissue progresses, lung function decreases, ultimately leading to respiratory compromise.
Furthermore, the presence of chrysotile fibers in lung tissue has been associated with malignancies. While the mechanism is not completely understood, it is believed that chronic irritation and cellular disruption from the retained fibers play a role in the development of cancers such as lung carcinoma and mesothelioma. Mesothelioma, although relatively rare, is highly associated with asbestos exposure, and chrysotile has been identified as a cause.
The cumulative effect of chrysotile fiber retention in the lungs is compounded over time. Long-term exposure increases the likelihood of developing chronic lung conditions or malignancies. This aspect underscores the necessity for proper occupational safety measures in industries where asbestos exposure is a hazard, as well as the critical need for the safe removal and disposal of materials containing chrysotile in renovation and demolition settings.
Continued research and surveillance are crucial to fully understand the long-term implications of chrysotile fiber inhalation. Monitoring of exposed individuals and populations is essential to developing improved risk assessment and management strategies. While the ongoing goal is to minimize exposure to these fibers, much remains to be done to ameliorate the effects on individuals with past and ongoing exposure, stressing the importance of combining scientific understanding with effective public health interventions.
Health Risks and Exposure Limits
The established health risks beyond the well-documented link to mesothelioma and lung cancer are multifaceted. Chronic inhalation of chrysotile fibers can lead to a disease known as asbestosis, a progressive pulmonary fibrosis caused by the scarring of lung tissue. This condition results from the body’s continuous and unsuccessful efforts to expel these fibers, leading to difficulty in breathing, persistent cough, and an increased risk of various pulmonary issues. The latency period—the time between exposure and the onset of disease—can stretch over several decades, making the exposure effects insidious and difficult to trace back to their origin.
Safe exposure limits for chrysotile asbestos have been established by various regulatory bodies around the world, yet they are not uniform and are subject to revision based on emerging scientific evidence. The Occupational Safety and Health Administration (OSHA) in the United States, for instance, has set permissible exposure limits (PELs) to 0.1 fibers per cubic centimeter of air as an eight-hour time-weighted average. Meanwhile, the National Institute for Occupational Safety and Health (NIOSH) recommends a more stringent exposure limit of 0.1 fibers per cubic centimeter as a recommended exposure limit (REL).
Despite these guidelines, the complexity of individual susceptibility and variations in fiber size and type implies that no level of exposure can be considered entirely “safe.” Furthermore, it is paramount to emphasize that chrysotile asbestos, regardless of its distinct properties compared to amphibole asbestos, shares a comparable ability to cause harm upon inhalation. Regulatory agencies and health professionals advocate for a continued reduction in permissible exposure limits and, when feasible, the elimination of exposure altogether, in alignment with the current global initiative to phase out asbestos use in favor of safer alternatives.
Moreover, beyond the exposure limits set for occupational settings, the general public should also be aware of potential exposure risks from aging buildings and infrastructure that may still contain asbestos. While undisturbed, well-contained asbestos may present minimal risk, renovation, demolition, or damage can release fibers into the surrounding environment. Thus, strict adherence to safety protocols and the employment of specialists for the handling and disposal of such materials are necessitated to prevent inadvertent exposure.
Continued vigilance and research in the field of occupational and environmental health is essential to refine our understanding of asbestos-related diseases and improve upon the regulatory frameworks. Addressing the residual presence of chrysotile asbestos remains a public health imperative, requiring collaborative efforts between industry, governments, and health agencies to mitigate risks and enhance the safety of living and working environments.
Modern Strategies for Enhanced Clearance
Emerging Strategies for Chrysotile Clearance from the Lungs
In recent years, researchers have initiated novel approaches to augment the body’s capacity to clear chrysotile fibers from the pulmonary system. We will now delve into a selection of promising strategies currently under scientific exploration.
One such strategy involves pharmacological agents designed to boost the effectiveness of the mucociliary escalator. By thickening the mucus or increasing the beat frequency of cilia, these agents may potentially enhance the clearance of small chrysotile fibers, which might otherwise slip through this natural defense mechanism.
Another cutting-edge area of investigation is the potential use of inhaled corticosteroids. This class of drugs, traditionally used for controlling inflammation in chronic respiratory diseases, may also attenuate the inflammatory response induced by chrysotile fibers. Reduction of inflammation may, in turn, facilitate the removal of fibers and mitigate the formation of scar tissue.
Moreover, biotechnological developments have led to exploration into genetic therapies. These aim to enhance the intrinsic capacity of alveolar macrophages to phagocytose or ‘eat’ foreign particles, including chrysotile fibers. Elevating the macrophages’ digestive efficiency could be revolutionary, leading to a significant reduction in fiber retention and associated pulmonary damage.
Furthermore, the advent of nanoparticle technology offers a beacon of hope. Magnetic nanoparticles, when guided by an external magnetic field, could potentially bind to chrysotile fibers, thereby allowing their guided removal from the lung passages. While still in the experimental phase, the premise of using nanotechnology opens a landscape of possibilities in treating asbestos-related conditions.
Stem cell therapy, a frontier of medical science, has been proposed as a method to repair lung tissue damaged by chrysotile fibers. Through the introduction of stem cells, the goal would be to regenerate healthy lung tissue, thereby enhancing both the clearance of fibers and the overall respiratory health of the individual.
It is crucial to underscore that while these strategies are pioneers in their respective fields, they are yet to be established in clinical practice. Much research, experimentation, and validation lie ahead. The collaboration between interdisciplinary teams in elucidating the mechanisms, efficacy, and safety of these approaches cannot be overstressed, as the overarching aim is to reduce the burden of asbestos-related diseases and improve the quality of life of those affected.
In the interim, emphasis remains on adhering to robust occupational safety measures, implementing strict environmental regulations, and ensuring proper management of asbestos-contaminated sites. As science presses forward, optimistic that it is within reach to transform the prognosis for individuals exposed to chrysotile asbestos, it is incumbent upon researchers, healthcare professionals, and policymakers to forge a path towards a future where lung health can be preserved despite prior asbestos exposure.
The delicate interplay between the body’s attempts to purge the invasive chrysotile fibers and the steady advancement of medical interventions plays a pivotal role in shaping our ongoing narrative with this formidable mineral. Through relentless research and innovation, strides in medical science persist in the search for solutions to enhance pulmonary clearance and address the health consequences associated with asbestos exposure. As we consider the collective wisdom gleaned from toxicological and epidemiological studies, along with the robust debates surrounding exposure limits, we must remain ever vigilant, ensuring that our engagements with materials like chrysotile are informed by the lessons of the past and guided by a commitment to public health and safety in the future.